Miscarriage
| Miscarriage | |
|---|---|
| Classification and external resources | |
| ICD-10 | O03. |
| ICD-9 | 634 |
| MedlinePlus | 001488 |
| eMedicine | topic list |
| MeSH | D000022 |
Miscarriage or spontaneous abortion is the spontaneous end of a pregnancy at a stage where the embryo or fetus is incapable of surviving, generally defined in humans at prior to 24 weeks of gestation. Miscarriage is the most common complication of early pregnancy.[1]
Contents |
Terminology
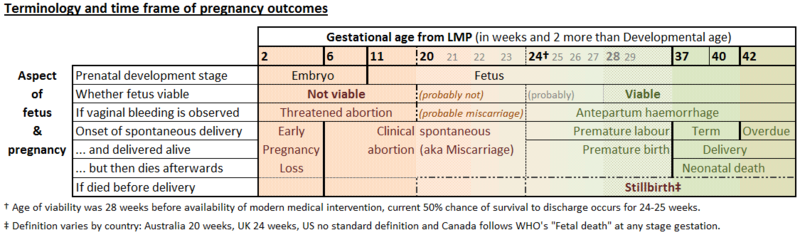
Very early miscarriages—those that occur before the sixth week LMP (since the woman's Last Menstrual Period)—are medically termed early pregnancy loss[2] or chemical pregnancy.[3] Miscarriages that occur after the sixth week LMP are medically termed clinical spontaneous abortion.[2]
In medical contexts, the word "abortion" refers to any process by which a pregnancy ends with the death and removal or expulsion of the fetus, regardless of whether it is spontaneous or intentionally induced. Many women who have had miscarriages, however, object to the term "abortion" in connection with their experience, as it is generally associated with induced abortions. In recent years there has been discussion in the medical community about avoiding the use of this term in favor of the less ambiguous term "miscarriage".[4]
Labour resulting in live birth before the 37th week of pregnancy is termed "premature birth", even if the infant dies shortly afterward. The limit of viability at which 50% of fetus/infants survive longterm is around 24 weeks, with moderate or major neurological disability dropping to 50% only by 26 weeks.[5] Although long-term survival has never been reported for infants born from pregnancy shorter than 21 weeks and 5 days,[6] infants born as early as the 16th week of pregnancy may sometimes live for some minutes after birth.[7]
A fetus that dies while in the uterus after about the 20–24th week of pregnancy is termed a "stillbirth"; the precise gestational age definition varies by country. Premature births or stillbirths are not generally considered miscarriages, though usage of the terms and causes of these events may overlap.
Miscarriage of a fetus is also called intrauterine fetal death (IUFT).
Classification
The clinical presentation of a threatened abortion describes any bleeding seen during pregnancy prior to viability, that has yet to be assessed further. At investigation it may be found that the fetus remains viable and the pregnancy continues without further problems. It has been suggested that bed rest improves the chances of the pregnancy continuing when a small subchorionic hematoma has been found on ultrasound scans.[8]
Alternatively the following terms are used to describe pregnancies that do not continue:
- An empty sac is a condition where the gestational sac develops normally, while the embryonic part of the pregnancy is either absent or stops growing very early. Other terms for this condition are blighted ovum and anembryonic pregnancy.
- An inevitable abortion describes where the cervix has already dilated open,[9] but the fetus has yet to be expelled. This usually will progress to a complete abortion. The fetal heart beat may have been shown to have stopped, but this is not part of the criteria.
- A complete abortion is when all products of conception have been expelled. Products of conception may include the trophoblast, chorionic villi, gestational sac, yolk sac, and fetal pole (embryo); or later in pregnancy the fetus, umbilical cord, placenta, amniotic fluid, and amniotic membrane.
- An incomplete abortion occurs when tissue has been passed, but some remains in utero.[10]
- A missed abortion is when the embryo or fetus has died, but a miscarriage has not yet occurred. It is also referred to as delayed or missed miscarriage.
The following two terms consider wider complications or implications of a miscarriage:
- A septic abortion occurs when the tissue from a missed or incomplete abortion becomes infected. The infection of the womb carries risk of spreading infection (septicaemia) and is a grave risk to the life of the woman.
- Recurrent pregnancy loss (RPL) or recurrent miscarriage (medically termed habitual abortion) is the occurrence of three consecutive miscarriages. If the proportion of pregnancies ending in miscarriage is 15%,[11] then the probability of two consecutive miscarriages is 2.25% and the probability of three consecutive miscarriages is 0.34%. The occurrence of recurrent pregnancy loss is 1%.[11] A large majority (85%) of women who have had two miscarriages will conceive and carry normally afterwards.
The physical symptoms of a miscarriage vary according to the length of pregnancy:[12]
- At up to six weeks only small blood clots may be present, possibly accompanied by mild cramping or period pain.
- At 6 to 13 weeks a clot will form around the embryo or fetus, and the placenta, with many clots up to 5 cm in size being expelled prior to a completed miscarriage. The process may take a few hours or be on and off for a few days. Symptoms vary widely and can include vomiting and loose bowels, possibly due to physical discomfort.
- At over 13 weeks the fetus may be easily passed from the womb, however the placenta is more likely to be fully or partially retained in the uterus, resulting in an incomplete abortion. The physical signs of bleeding, cramping and pain can be similar to an early miscarriage, but sometimes more severe and labour-like.
Signs and symptoms
The most common symptom of a miscarriage is bleeding;[13] bleeding during pregnancy may be referred to as a threatened abortion. Of women who seek clinical treatment for bleeding during pregnancy, about half will go on to have a miscarriage.[14] Symptoms other than bleeding are not statistically related to miscarriage.[13]
Miscarriage may also be detected during an ultrasound exam, or through serial human chorionic gonadotropin (HCG) testing. Women pregnant from ART methods, and women with a history of miscarriage, may be monitored closely and so detect a miscarriage sooner than women without such monitoring.
Several medical options exist for managing documented nonviable pregnancies that have not been expelled naturally.
Psychological
Although a woman physically recovers from a miscarriage quickly, psychological recovery for parents in general can take a long time. People differ greatly in this regard: some are able to move on after a few months, but others take more than a year. Still others may feel relief or other less negative emotions. A questionnaire (GHQ-12 General Health Questionnaire) study following women having miscarried showed that half (55%) of the miscarrying women presented with significant psychological distress immediately, 25% at 3 months; 18% at 6 months, and 11% at 1 year after miscarriage.[15]

For those who do go through a process of grief, it is often as if a baby had been born but died. How short a time the fetus lived in the womb may not matter for the feeling of loss. From the moment pregnancy is discovered, the parents can start to bond with the embryo or fetus. When the pregnancy turns out not to be viable, dreams, fantasies and plans for the future are disturbed roughly.
Besides the feeling of loss, a lack of understanding by others is often important. People who have not experienced a miscarriage themselves may find it hard to empathize with what has occurred and how upsetting it may be. This may lead to unrealistic expectations of the parents' recovery. The pregnancy and miscarriage are hardly mentioned any more in conversation, often because the subject is too painful. This can make the woman feel particularly isolated. Inappropriate or insensitive responses from the medical profession can add to the distress and trauma experienced, so in some cases attempts have been made to draw up a standard code of practice.[16]
Interaction with pregnant women and newborn children is often also painful for parents who have experienced miscarriage. Sometimes this makes interaction with friends, acquaintances and family very difficult.[17]
Causes
Miscarriages can occur for many reasons, not all of which can be identified. Some of these causes include genetic, uterine or hormonal abnormalities, reproductive tract infections, and tissue rejection.
First trimester

Most clinically apparent miscarriages (two thirds to three-quarters in various studies) occur during the first trimester.[18][19]
Chromosomal abnormalities are found in more than half of embryos miscarried in the first 13 weeks. A pregnancy with a genetic problem has a 95% probability of ending in miscarriage. Most chromosomal problems happen by chance, have nothing to do with the parents, and are unlikely to recur. Chromosomal problems due to a parent's genes is, however, a possibility. This is more likely to have been the cause in the case of repeated miscarriages, or if one of the parents has a child or other relatives with birth defects.[20] Genetic problems are more likely to occur with older parents; this may account for the higher miscarriage rates observed in older women.[21]
Another cause of early miscarriage may be progesterone deficiency. Women diagnosed with low progesterone levels in the second half of their menstrual cycle (luteal phase) may be prescribed progesterone supplements, to be taken for the first trimester of pregnancy.[20] However, no study has shown that general first-trimester progesterone supplements reduce the risk of miscarriage,[22] and even the identification of problems with the luteal phase as contributing to miscarriage has been questioned.[23]
Second trimester
Up to 15% of pregnancy losses in the second trimester may be due to uterine malformation, growths in the uterus (fibroids), or cervical problems.[20] These conditions may also contribute to premature birth.[18]
One study found that 19% of second trimester losses were caused by problems with the umbilical cord. Problems with the placenta may also account for a significant number of later-term miscarriages.[24]
General risk factors
Pregnancies involving more than one fetus are at increased risk of miscarriage.[20]
Uncontrolled diabetes greatly increases the risk of miscarriage. Women with controlled diabetes are not at higher risk of miscarriage. Because diabetes may develop during pregnancy (gestational diabetes), an important part of prenatal care is to monitor for signs of the disease.[20]
Polycystic ovary syndrome is a risk factor for miscarriage, with 30-50% of pregnancies in women with PCOS being miscarried in the first trimester. Two studies have shown treatment with the drug metformin to significantly lower the rate of miscarriage in women with PCOS (the metformin-treated groups experienced approximately one-third the miscarriage rates of the control groups).[25] However, a 2006 review of metformin treatment in pregnancy found insufficient evidence of safety and did not recommend routine treatment with the drug.[26]
High blood pressure during pregnancy, known as preeclampsia, is sometimes caused by an inappropriate immune reaction to the developing fetus, and is associated with the risk of miscarriage. Similarly, women with a history of recurrent miscarriages are at risk of developing preeclampsia.[27]
Severe cases of hypothyroidism increase the risk of miscarriage. The effect of milder cases of hypothyroidism on miscarriage rates has not been established. The presence of certain immune conditions such as autoimmune diseases is associated with a greatly increased risk of miscarriage.[20]
Certain illnesses (such as rubella, chlamydia and others) increase the risk of miscarriage.[20]
Tobacco (cigarette) smokers have an increased risk of miscarriage.[28] An increase in miscarriage is also associated with the father being a cigarette smoker.[2] The husband study observed a 4% increased risk for husbands who smoke less than 20 cigarettes/day, and an 81% increased risk for husbands who smoke 20 or more cigarettes/day.
Cocaine use increases miscarriage rates.[28] Physical trauma, exposure to environmental toxins, and use of an IUD during the time of conception have also been linked to increased risk of miscarriage.[29]
Antidepressants specially paroxetine and venlafaxine can lead to spontaneous abortion.[30][31]

The age of the mother is a major risk factor. Miscarriage rates grow at an ever-increasing rate after age 20. [32][33]
Suspected risk factors
Several factors have been correlated with higher miscarriage rates, but whether they cause miscarriages is debated. No causal mechanism may be known, the studies showing a correlation may have been retrospective (beginning the study after the miscarriages occurred, which can introduce bias) rather than prospective (beginning the study before the women became pregnant), or both.
Nausea and vomiting of pregnancy (NVP, or morning sickness) are associated with a decreased risk of miscarriage. Several mechanisms have been proposed for this relationship, but none are widely agreed on.[34] Because NVP may alter a woman's food intake and other activities during pregnancy, it may be a confounding factor when investigating possible causes of miscarriage.
One such factor is exercise. A study of over 92,000 pregnant women found that most types of exercise (with the exception of swimming) correlated with a higher risk of miscarriage prior to 18 weeks. Increasing time spent on exercise was associated with a greater risk of miscarriage: an approximately 10% increased risk was seen with up to 1.5 hours per week of exercise, and a 200% increased risk was seen with over 7 hours per week of exercise. High-impact exercise was especially associated with the increased risk. No relationship was found between exercise and miscarriage rates after the 18th week of pregnancy. The majority of miscarriages had already occurred at the time women were recruited for the study, and no information on nausea during pregnancy or exercise habits prior to pregnancy was collected.[35]
Caffeine consumption has also been correlated to miscarriage rates, at least at higher levels of intake. A 2007 study of over 1,000 pregnant women found that women who reported consuming 200 mg or more of caffeine per day experienced a 25% miscarriage rate, compared to 13% among women who reported no caffeine consumption. 200 mg of caffeine is present in 10 oz (300 mL) of coffee or 25 oz (740 mL) of tea. This study controlled for pregnancy-associated nausea and vomiting (NVP or morning sickness): the increased miscarriage rate for heavy caffeine users was seen regardless of how NVP affected the women. About half of the miscarriages had already occurred at the time women were recruited for the study.[36] A second 2007 study of approximately 2,400 pregnant women found that caffeine intake up to 200 mg per day was not associated with increased miscarriage rates (the study did not include women who drank more than 200 mg per day past early pregnancy).[37] A prospective cohort study in 2009 showed no increased risk.[38]
Diagnosis
A miscarriage can be confirmed via ultrasound and by the examination of the passed tissue. When looking for gross or microscopic pathologic symptoms of miscarriage, one looks for the products of conception. Microscopically, these include villi, trophoblast, fetal parts, and background gestational changes in the endometrium. Genetic tests may also be performed to look for abnormal chromosome arrangements.
Management
Blood loss during early pregnancy is the most common symptom of both miscarriage and of ectopic pregnancy. Pain does not strongly correlate with miscarriage, but is a common symptom of ectopic pregnancy.[13] In the case of concerning blood loss, pain, or both, transvaginal ultrasound is performed. If a viable intrauterine pregnancy is not found with ultrasound, serial βHCG tests should be performed to rule out ectopic pregnancy, which is a life-threatening situation.[39][40]
If the bleeding is light, making an appointment to see one's doctor is recommended. If bleeding is heavy, there is considerable pain, or there is a fever, then emergency medical attention is recommended to be sought.
No treatment is necessary for a diagnosis of complete abortion (as long as ectopic pregnancy is ruled out). In cases of an incomplete abortion, empty sac, or missed abortion there are three treatment options:
- With no treatment (watchful waiting), most of these cases (65–80%) will pass naturally within two to six weeks.[41] This path avoids the side effects and complications possible from medications and surgery.[42]
- Medical management usually consists of using misoprostol (a prostaglandin, brand name Cytotec) to encourage completion of the miscarriage. About 95% of cases treated with misoprostol will complete within a few days.[41]
- Surgical treatment (most commonly vacuum aspiration, sometimes referred to as a D&C or D&E) is the fastest way to complete the miscarriage. It also shortens the duration and heaviness of bleeding, and is the best treatment for physical pain associated with the miscarriage.[41] In cases of repeated miscarriage or later-term pregnancy loss, D&C is also the best way to obtain tissue samples for pathology examination. D&C, however, has a higher risk of complications, including risk of injury to the cervix and uterus, perforation of the uterus, and potential scarring of the intrauterine lining. This is an important consideration for women who would like to have children in the future and want to minimize the risk of damaging their uterus.
Epidemiology
Determining the prevalence of miscarriage is difficult. Many miscarriages happen very early in the pregnancy, before a woman may know she is pregnant. Treatment of women with miscarriage at home means medical statistics on miscarriage miss many cases.[14] Prospective studies using very sensitive early pregnancy tests have found that 25% of pregnancies are miscarried by the sixth week LMP (since the woman's Last Menstrual Period).[43][44] Clinical miscarriages (those occurring after the sixth week LMP) occur in 8% of pregnancies.[44]
The risk of miscarriage decreases sharply after the 10th week LMP, i.e. when the fetal stage begins.[45] The loss rate between 8.5 weeks LMP and birth is about two percent; loss is “virtually complete by the end of the embryonic period."[46]
The prevalence of miscarriage increases considerably with age of the parents. One study found that pregnancies from men younger than 25 years are 40% less likely to end in miscarriage than pregnancies from men 25–29 years. The same study found that pregnancies from men older than 40 years are 60% more likely to end in miscarriage than the 25–29-year age group.[47] Another study found that the increased risk of miscarriage in pregnancies from older men is mainly seen in the first trimester.[48] Yet another study found an increased risk in women, by the age of 45, on the order of 800% (compared to the 20–24 age group in that study), 75% of pregnancies ended in miscarriage.[49]
In other animals
Miscarriage occurs in all animals that experience pregnancy. There are a variety of known risk factors for miscarriage in non-human animals. For example, in sheep, it may be caused by crowding through doors, or being chased by dogs.[50] In cows, miscarriage (i.e. spontaneous abortion) may be caused by contagious disease, such as Brucellosis or Campylobacter, but can often be controlled by vaccination.[51] Other diseases are also known to target animals for miscarriage. Spontaneous abortion occurs in pregnant Prairie Voles when their mate is removed and they are exposed to a new male,[52] an example of the Bruce effect, although this effect is seen less in wild populations than in the laboratory.[53] Female mice that had spontaneous abortions showed a sharp rise in the time spent with unfamiliar males preceding the abortion.[54]
ICD10 codes
|
N96 |
See also
- Abortion
- Childbirth
- Stillbirth
- Premature birth
References
- ↑ Petrozza, John C (August 29, 2006). "Early Pregnancy Loss". eMedicine. WebMD. http://www.emedicine.com/med/topic3241.htm. Retrieved 20 July 2007.
"Early Pregnancy Loss (Miscarriage)". Pregnancy-bliss.co.uk. The Daily Telegraph. 2007. http://www.pregnancy-bliss.co.uk/miscarriage.html. Retrieved 20 July 2007. - ↑ 2.0 2.1 2.2 Venners S, Wang X, Chen C, Wang L, Chen D, Guang W, Huang A, Ryan L, O'Connor J, Lasley B, Overstreet J, Wilcox A, Xu X (2004). "Paternal smoking and pregnancy loss: a prospective study using a biomarker of pregnancy.". Am J Epidemiol 159 (10): 993–1001. doi:10.1093/aje/kwh128. PMID 15128612. http://aje.oxfordjournals.org/cgi/content/full/159/10/993.
- ↑ "What is a chemical pregnancy?". Baby Hopes. http://www.babyhopes.com/articles/chemical-pregnancy.html. Retrieved 27 April 2007.
- ↑ Hutchon D, Cooper S (1998). "Terminology for early pregnancy loss must be changed". BMJ 317 (7165): 1081. PMID 9774309.
Hutchon D (1998). "Understanding miscarriage or insensitive abortion: time for more defined terminology?". Am. J. Obstet. Gynecol. 179 (2): 397–8. doi:10.1016/S0002-9378(98)70370-9. PMID 9731844. - ↑ Kaempf JW, Tomlinson M, Arduza C, et al. (2006). "Medical staff guidelines for periviability pregnancy counseling and medical treatment of extremely premature infants". Pediatrics 117 (1): 22–9. doi:10.1542/peds.2004-2547. PMID 16396856. http://pediatrics.aappublications.org/cgi/content/full/117/1/22. - in particular see TABLE 1 Survival and Neurologic Disability Rates Among Extremely Premature Infants
- ↑ "Powell's Books - Guinness World Records 2004 (Guinness Book of Records) by". http://www.powells.com/biblio?show=0553587129&page=excerpt?. Retrieved 28 November 2007.
- ↑ Patricia Lee June (November 2001). A Pediatrician Looks at Babies Late in Pregnancy and Late Term Abortion. Presbyterians Pro-Life. http://www.ppl.org/PJune_PostViability_2001.html. Retrieved 24 December 2006.
- ↑ Ben-Haroush A, Yogev Y, Mashiach R, Meizner I (2003). "Pregnancy outcome of threatened abortion with subchorionic hematoma: possible benefit of bed-rest?". Isr. Med. Assoc. J. 5 (6): 422–4. PMID 12841015.
- ↑ Kaufman, Matthew H.; Latha Stead; Feig, Robert (2007). First aid for the obstetrics & gynecology clerkship. New York: McGraw-Hill, Medical Pub. Division. pp. 138. ISBN 0-07-144874-8.
- ↑ MedlinePlus (25 October 2004). "Abortion - incomplete". Medical Encyclopedia. http://www.nlm.nih.gov/medlineplus/ency/article/000904.htm. Retrieved 24 May 2006.
- ↑ 11.0 11.1 Royal College of Obstetricians and Gynaecologists (May 2003). "The investigation and treatment of couples with recurrent miscarriage". Guideline No 17. http://www.guideline.gov/summary/summary.aspx?ss=15&doc_id=7681&nbr=4480. Retrieved 25 June 2009.
- ↑ "miscarriage". October 2004. http://www.birth.com.au/Info.asp?class=6620&page=13. Retrieved 0 March 2009.
- ↑ 13.0 13.1 13.2 Gracia C, Sammel M, Chittams J, Hummel A, Shaunik A, Barnhart K (2005). "Risk factors for spontaneous abortion in early symptomatic first-trimester pregnancies". Obstet Gynecol 106 (5 Pt 1): 993–9. doi:10.1097/01.AOG.0000183604.09922.e0 (inactive 2010-03-17). PMID 16260517.
- ↑ 14.0 14.1 Everett C (5 July 1997). "Incidence and outcome of bleeding before the 20th week of pregnancy: prospective study from general practice.". BMJ 315 (7099): 32–4. PMID 9233324. PMC 2127042. http://bmj.bmjjournals.com/cgi/content/full/315/7099/32.
- ↑ Lok IH, Yip AS, Lee DT, Sahota D, Chung TK (April 2010). "A 1-year longitudinal study of psychological morbidity after miscarriage". Fertil. Steril. 93 (6): 1966–75. doi:10.1016/j.fertnstert.2008.12.048. PMID 19185858.
- ↑ Miscarriage Standard Code of Practice
- ↑ David Vernon (2005). "Having a Great Birth in Australia". http://web.mac.com/david.vernon/iWeb/Having%20a%20Great%20Birth%20in%20Australia/Welcome%20-%20Great%20Birth.html.
- ↑ 18.0 18.1 Rosenthal, M. Sara (1999). "The Second Trimester". The Gynecological Sourcebook. WebMD. http://www.webmd.com/content/article/4/1680_51802.htm. Retrieved 18 December 2006.
- ↑ Francis O (1959). "An analysis of 1150 cases of abortions from the Government R.S.R.M. Lying-in Hospital, Madras". J Obstet Gynaecol India 10 (1): 62–70. PMID 12336441.
- ↑ 20.0 20.1 20.2 20.3 20.4 20.5 20.6 "Miscarriage: Causes of Miscarriage". HealthSquare.com. http://www.healthsquare.com/fgwh/wh1ch27p3.htm. Retrieved 18 September 2007.taken word-for-word from pp. 347-9 of: "Chapter 27. What To Do When Miscarriage Strikes". The PDR Family Guide to Women's Health and Prescription Drugs. Montvale, NJ: Medical Economics. 1994. pp. 345–50. ISBN 1-56363-086-9.
- ↑ "Pregnancy Over Age 30". MUSC Children's Hospital. http://www.musckids.com/health_library/hrpregnant/over30.htm. Retrieved 18 December 2006.
- ↑ Wahabi HA, Abed Althagafi NF, Elawad M (2007). "Progestogen for treating threatened miscarriage". Cochrane database of systematic reviews (Online) (3): CD005943. doi:10.1002/14651858.CD005943.pub2. PMID 17636813.
- ↑ Bukulmez O, Arici A (2004). "Luteal phase defect: myth or reality". Obstet. Gynecol. Clin. North Am. 31 (4): 727–44, ix. doi:10.1016/j.ogc.2004.08.007. PMID 15550332.
- ↑ Peng H, Levitin-Smith M, Rochelson B, Kahn E (2006). "Umbilical cord stricture and overcoiling are common causes of fetal demise.". Pediatr Dev Pathol 9 (1): 14–9. doi:10.2350/05-05-0051.1. PMID 16808633.
- ↑ Jakubowicz DJ, Iuorno MJ, Jakubowicz S, Roberts KA, Nestler JE (2002). "Effects of metformin on early pregnancy loss in the polycystic ovary syndrome". J. Clin. Endocrinol. Metab. 87 (2): 524–9. doi:10.1210/jc.87.2.524. PMID 11836280. http://jcem.endojournals.org/cgi/content/full/87/2/524. Retrieved 17 July 2007.
Khattab S, Mohsen IA, Foutouh IA, Ramadan A, Moaz M, Al-Inany H (2006). "Metformin reduces abortion in pregnant women with polycystic ovary syndrome". Gynecol. Endocrinol. 22 (12): 680–4. doi:10.1080/09513590601010508. PMID 17162710. - ↑ Lilja AE, Mathiesen ER (2006). "Polycystic ovary syndrome and metformin in pregnancy". Acta obstetricia et gynecologica Scandinavica 85 (7): 861–8. doi:10.1080/00016340600780441. PMID 16817087.
- ↑ "The effect of recurrent miscarriage and infertility on the risk of pre-eclampsia."; Trogstad L, Magnus P, Moffett A, Stoltenberg C.; BJOG: An International Journal of Obstetrics & Gynaecology, Volume 116 Issue 1, pp. 108–113; http://www.ncbi.nlm.nih.gov/pubmed/19087081
- ↑ 28.0 28.1 Ness R, Grisso J, Hirschinger N, Markovic N, Shaw L, Day N, Kline J (1999). "Cocaine and tobacco use and the risk of spontaneous abortion.". N Engl J Med 340 (5): 333–9. doi:10.1056/NEJM199902043400501. PMID 9929522.
- ↑ "Miscarriage: An Overview". Armenian Medical Network. 2005. http://www.health.am/pregnancy/more/miscarriage_an_overview/. Retrieved 19 September 2007.
- ↑ PMID 19863482 (PubMed)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand - ↑ PMID 20513781 (PubMed)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand - ↑ Heffner L. Advanced, Maternal Age – How old is too old? New England Journal of Medicine 2004; 351(19):1927–29.
- ↑ http://www.endo.gr/cgi/reprint/351/19/1927.pdf
- ↑ Furneaux EC, Langley-Evans AJ, Langley-Evans SC (2001). "Nausea and vomiting of pregnancy: endocrine basis and contribution to pregnancy outcome". Obstet Gynecol Surv 56 (12): 775–82. doi:10.1097/00006254-200112000-00004. PMID 11753180.
- ↑ Madsen M, Jørgensen T, Jensen ML, et al. (2007). "Leisure time physical exercise during pregnancy and the risk of miscarriage: a study within the Danish National Birth Cohort". BJOG 114 (11): 1419–26. doi:10.1111/j.1471-0528.2007.01496.x. PMID 17877774.
- ↑ Weng X, Odouli R, Li DK (2008). "Maternal caffeine consumption during pregnancy and the risk of miscarriage: a prospective cohort study". Am J Obstet Gynecol 198 (3): 279.e1–8. doi:10.1016/j.ajog.2007.10.803. PMID 18221932.
Grady, Denise (January 20, 2008). "Study Sees Caffeine Possibly Tied to Miscarriages". The New York Times. http://www.nytimes.com/2008/01/20/health/20cnd-caffeine.html?_r=1&bl&ex=1201150800&en=0019b93b4bb1c219&ei=5087%0A. Retrieved 23 January 2008. - ↑ Savitz DA, Chan RL, Herring AH, Howards PP, Hartmann KE (January 2008). "Caffeine and miscarriage risk" (PDF). Epidemiology 19 (1): 55–62. doi:10.1097/EDE.0b013e31815c09b9. PMID 18091004. http://www.cafeesaude.com.br/downloads/caffeine%20miscarriage%202008%20A.pdf.
"Studies Examine Effects Of Caffeine Consumption On Miscarriage Risk". Medical News Today. 23 January 2008. http://www.medicalnewstoday.com/articles/94764.php. Retrieved 16 February 2008. - ↑ Pollack AZ, Buck Louis GM, Sundaram R, Lum KJ (September 2009). "Caffeine consumption and miscarriage: a prospective cohort study". Fertil. Steril. 93 (1): 304–6. doi:10.1016/j.fertnstert.2009.07.992. PMID 19732873.
- ↑ Yip S, Sahota D, Cheung L, Lam P, Haines C, Chung T (2003). "Accuracy of clinical diagnostic methods of threatened abortion". Gynecol Obstet Invest 56 (1): 38–42. doi:10.1159/000072482. PMID 12876423.
- ↑ Condous G, Okaro E, Khalid A, Bourne T (2005). "Do we need to follow up complete miscarriages with serum human chorionic gonadotrophin levels?". BJOG 112 (6): 827–9. doi:10.1111/j.1471-0528.2004.00542.x. PMID 15924545.
- ↑ 41.0 41.1 41.2 Kripke C (2006). "Expectant management vs. surgical treatment for miscarriage". Am Fam Physician 74 (7): 1125–6. PMID 17039747. http://www.aafp.org/afp/20061001/cochrane.html#c2. Retrieved 31 December 2006.
- ↑ Tang O, Ho P (2006). "The use of misoprostol for early pregnancy failure.". Curr Opin Obstet Gynecol 18 (6): 581–6. doi:10.1097/GCO.0b013e32800feedb. PMID 17099326.
- ↑ Wilcox AJ, Baird DD, Weinberg CR (1999). "Time of implantation of the conceptus and loss of pregnancy.". New England Journal of Medicine 340 (23): 1796–1799. doi:10.1056/NEJM199906103402304. PMID 10362823.
- ↑ 44.0 44.1 Wang X, Chen C, Wang L, Chen D, Guang W, French J (2003). "Conception, early pregnancy loss, and time to clinical pregnancy: a population-based prospective study.". Fertil Steril 79 (3): 577–84. doi:10.1016/S0015-0282(02)04694-0. PMID 12620443.
- ↑ Q&A: Miscarriage. (August 6 , 2002). BBC News. Retrieved January 17, 2007. Also see Lennart Nilsson, A Child is Born 91 (1990)(At eight weeks, "the danger of a miscarriage . . . diminishes sharply.")
- ↑ Rodeck, Charles; Whittle, Martin. Fetal Medicine: Basic Science and Clinical Practice (Elsevier Health Sciences 1999), page 835.
- ↑ Kleinhaus K, Perrin M, Friedlander Y, Paltiel O, Malaspina D, Harlap S (2006). "Paternal age and spontaneous abortion". Obstet Gynecol 108 (2): 369–77. doi:10.1097/01.AOG.0000224606.26514.3a (inactive 26 June 2008). PMID 16880308.
- ↑ Slama R, Bouyer J, Windham G, Fenster L, Werwatz A, Swan S (2005). "Influence of paternal age on the risk of spontaneous abortion.". Am J Epidemiol 161 (9): 816–23. doi:10.1093/aje/kwi097. PMID 15840613.
- ↑ Nybo Andersen A, Wohlfahrt J, Christens P, Olsen J, Melbye M (2000). "Maternal age and fetal loss: population based register linkage study". BMJ 320 (7251): 1708–12. doi:10.1136/bmj.320.7251.1708. PMID 10864550.
- ↑ Spencer, James. Sheep Husbandry in Canada, page 124 (1911).
- ↑ "Beef cattle and Beef production: Management and Husbandry of Beef Cattle”, Encyclopaedia of New Zealand (1966).
- ↑ Fraser-Smith, AC (1975). "Male-induced pregnancy termination in the prairie vole, Microtus ochrogaster". Science (American Association for the Advancement of Science) 187 (4182): 1211–1213. doi:10.1126/science.1114340. PMID 1114340. http://www.sciencemag.org/cgi/content/abstract/187/4182/1211.
- ↑ Wolff, Jerry O; Wolff, Jerry (June 2002). "A field test of the Bruce effect in the monogamous prairie vole (Microtus ochrogaster)". Behavioral Ecology and Sociobiology (Berlin/Heidelberg: Springer) 52 (1): 31–7. doi:10.1007/s00265-002-0484-0. ISSN 1432-0762. http://www.springerlink.com/content/g65dcacncm0rwbkm/.
- ↑ Becker, Stuart D; Jane L Hurst (February 25, 2009 (online) / 7 May 2009). "Female behaviour plays a critical role in controlling murine pregnancy block". Proc. R. Soc. B (London: The Royal Society) 276 (1662): 1723–9. doi:10.1098/rspb.2008.1780. ISSN 1471-2945. PMID 19324836. PMC 2660991. http://rspb.royalsocietypublishing.org/content/early/2009/02/21/rspb.2008.1780.abstract.
External links
|
|||||||||||||||||||||||||||||||||||||||||||||